





心电图(ECG或者EKG)是利用心电图机从体表记录心脏每一心动周期所产生的电活动变化图形的技术。
心电图可以帮助诊断心律失常、心肌缺血、心肌梗死、心脏扩大、肥厚等病症。心电图的诊断应包括主导心律、心律失常和异常心电图的诊断。作为临床医师一定要自己会看图并结合临床分析,方能明确心电图改变的临床特点。
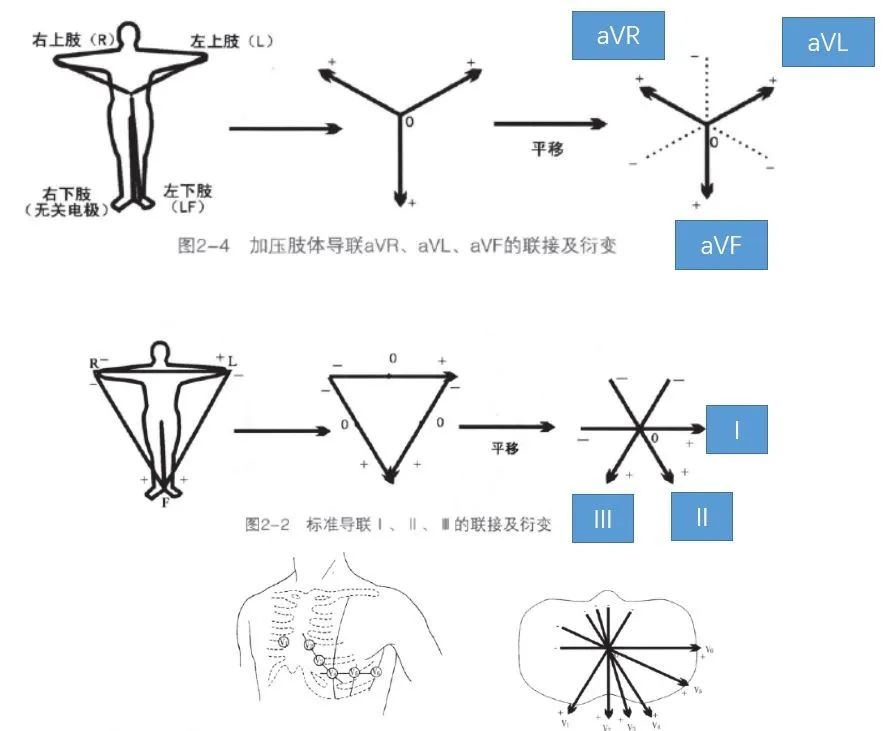
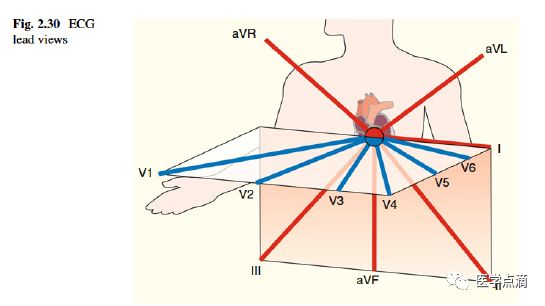
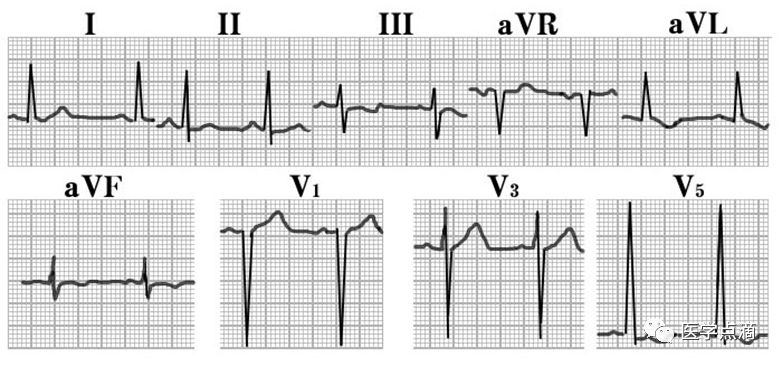
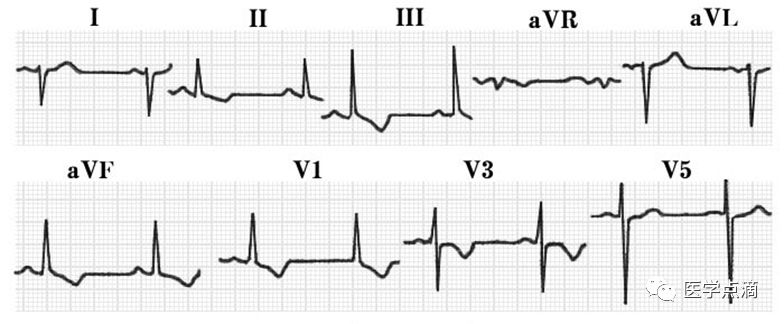
常规导联位置

心电图阅读(三步走)

-
形成初步印象(宽、窄、快、慢)
-
节律和心率(窦性P波) -
形态、电压、时相 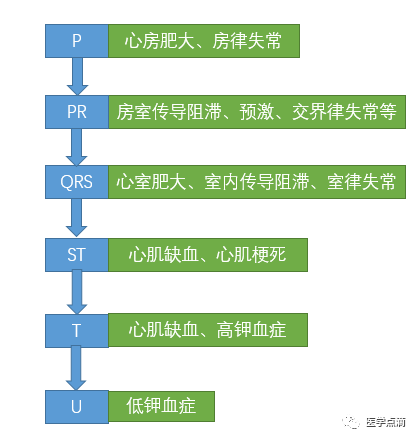
心 律

-
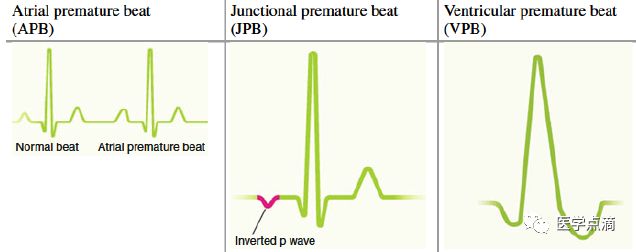
房性:房早(提前的1-2个P 波)【房早打乱窦房结的节奏,要重排,往往致使代偿间期不完全,P2-P 间距(早搏间期)+P -P4间距(代偿间期)≠2×任一窦PP间期】,房速(提前的3个以上的P 波),房扑、房颤(P波消失) -
交界性:(逆行P 波)(前传:P -R<0.12s;逆传:R-P <0.20s;实为P 波与QRS波之间的叠加关系,无从属关系。实际上,交界性早搏并无P -R间期或R-P 间期而言)(若R-P 间期>0.20s,P 波就可能不是房室结电指令逆传上去心房所产生的)【可以代偿间期不完全,也可以代偿间期完全(若逆传不到心房或不能沿结间束逆传,则对窦房结构不成威胁)】 -
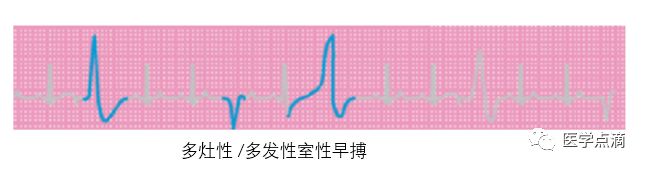
室性:提早出现宽大、畸形的QRS波(往往是代偿间期完全的)(窦性P波往往隐藏在QRS-T波群中,不下传的原因是室早逆传时造成房室结不应期)
-
主动性心律失常:“早搏”(主动性、抢先、快速型) -
被动性心律失常:“逸搏”(被动性、推迟、缓慢型) -
【窄QRS波:室上性;宽QRS波:室性】
-
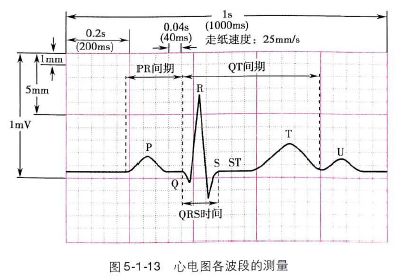
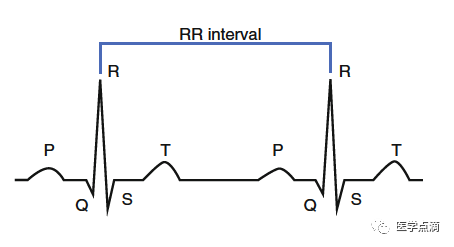
心律整齐时,心率=60/R-R间期(或P-P间期) -
心律不齐时,6秒内的心动周期数×10
-
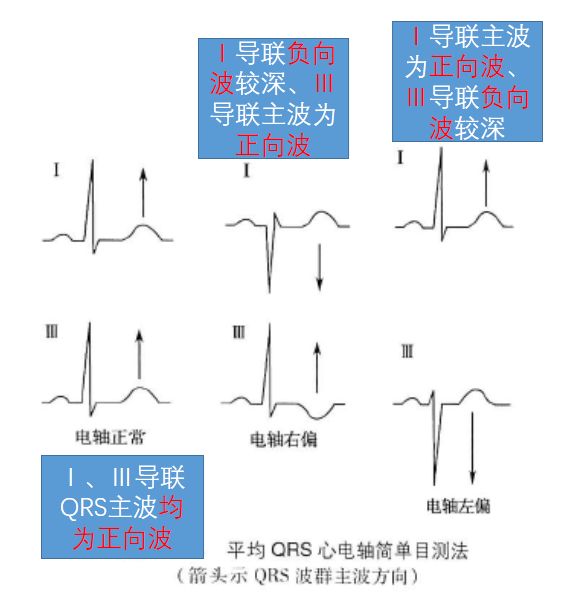
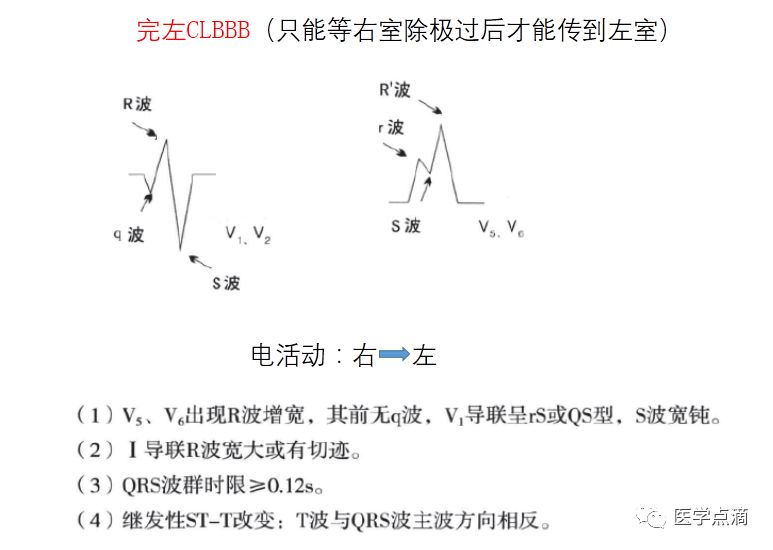
右偏:右心室肥厚,右束支传导阻滞 左偏:左心室肥厚,左束支传导阻滞,左前分支传导阻滞
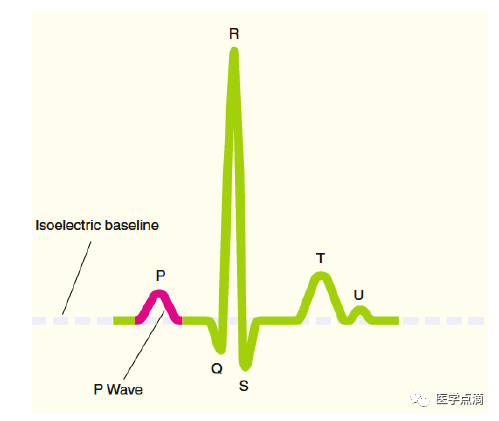
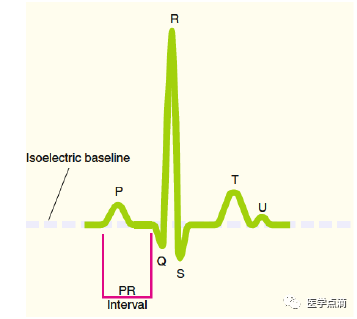
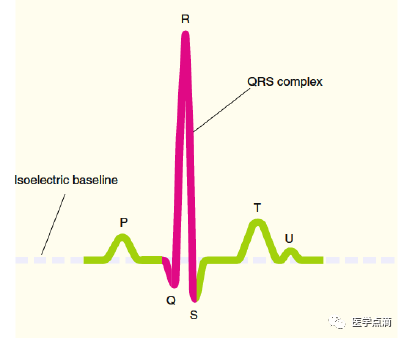
P 波

-
P波直立(Ⅰ、Ⅱ、aVF、V4-6 ) -
P波倒置(aVR) -
形态:宽(左房增大),高尖(右房增大) 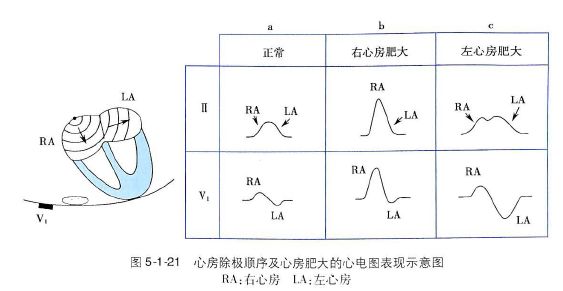
-
电压:<0.25mV(肢体),<0.20mV(胸前) -
时相:<0.12s(3小格)
-
生理性延迟作用 -
滤过作用【通常只能让200次/分的电冲动通过(偶尔可更多)】【房扑、房颤(心房率250-600次/分)等快速型室上性心律失常中滤过作用表现突出】
-
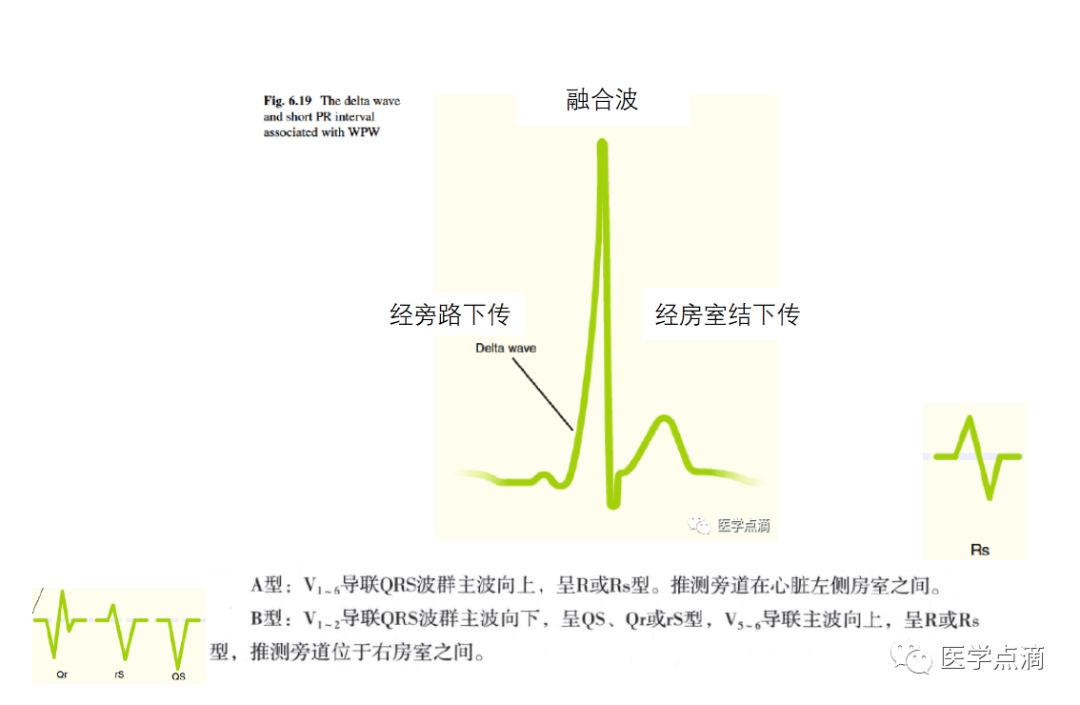
PR缩短<0.12s:预激(旁路);P波在QRS前面的交界性心律失常 -
PR延长>0.20s:Ⅰ度房室传导阻滞;P波在QRS前面的交界性心律失常 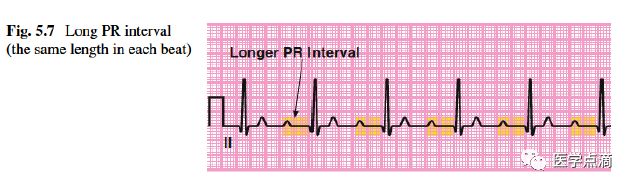
-
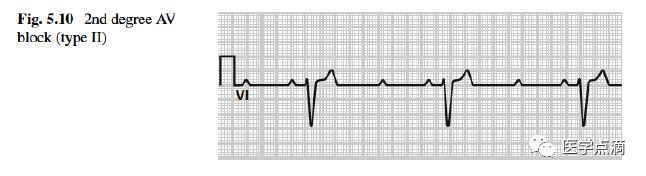
P波后R波脱落:Ⅱ度或者高度房室传导阻滞 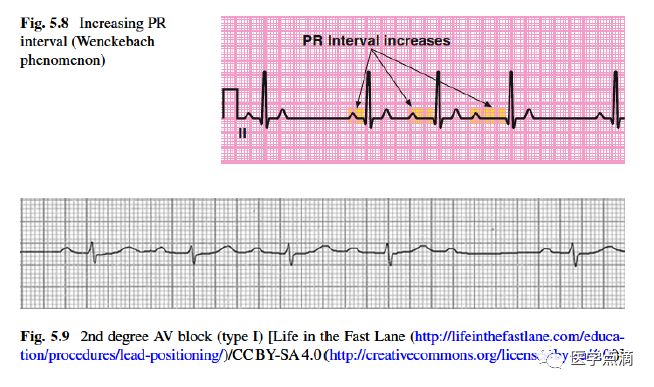
-
P波与QRS波无关系:Ⅲ度房室传导阻滞 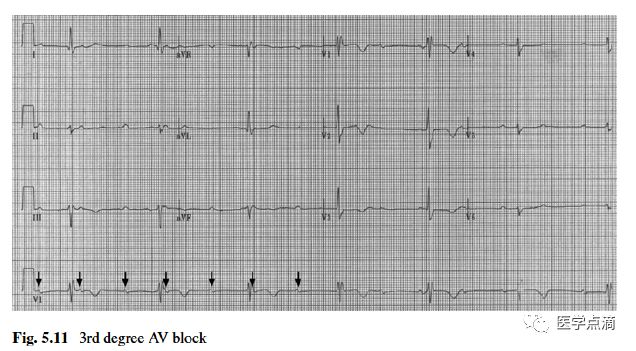
-
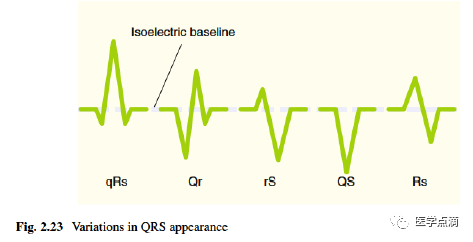
QRS波电压:RV5 高,左心室肥大;RV1 高,右心室肥大。 -
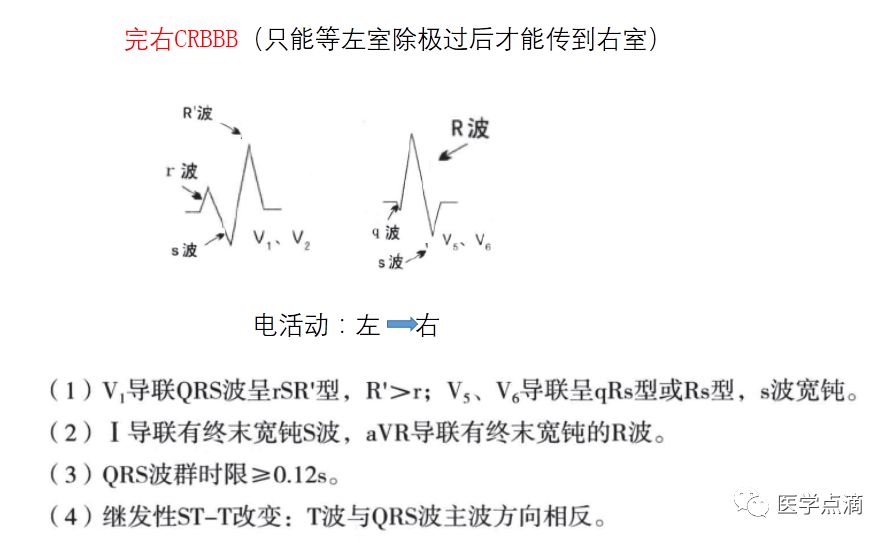
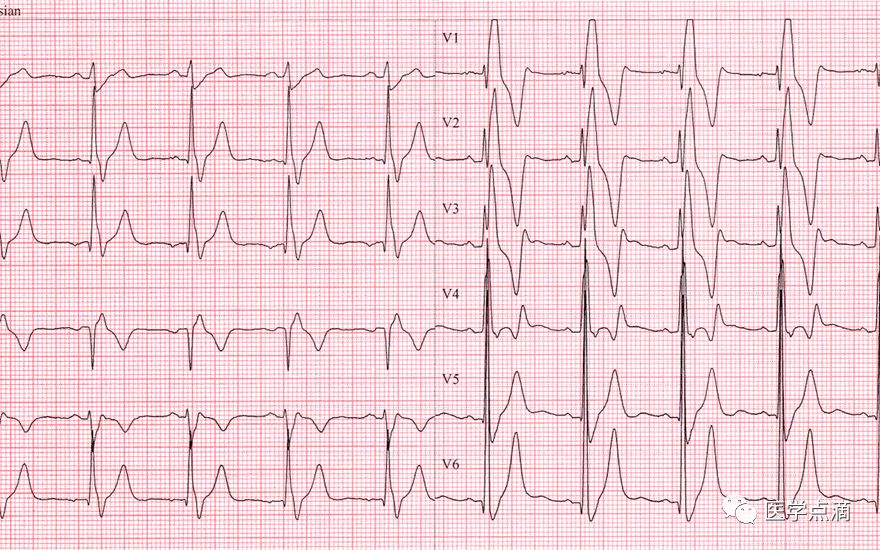
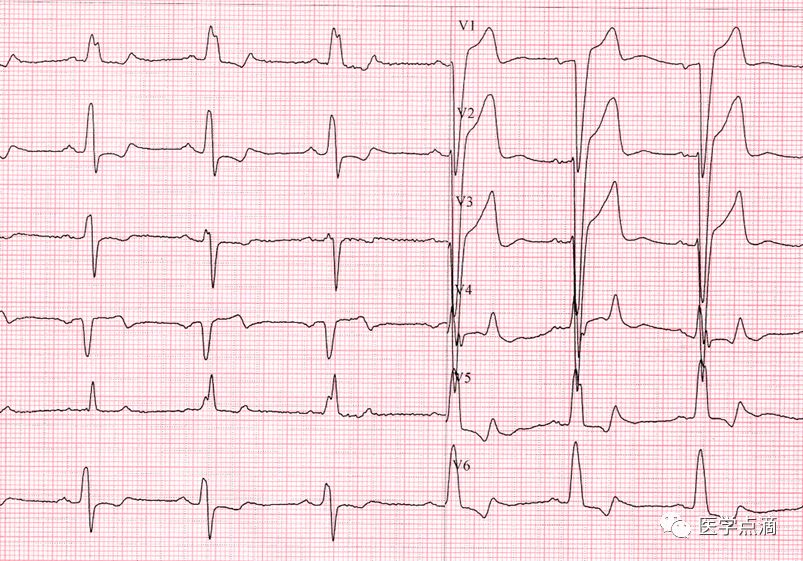
QRS波时限:束支传导阻滞 -
Q波:心肌梗死 -
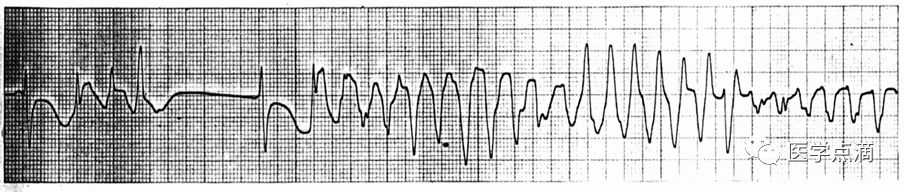
室性心律失常:室早,室速
左室肥厚

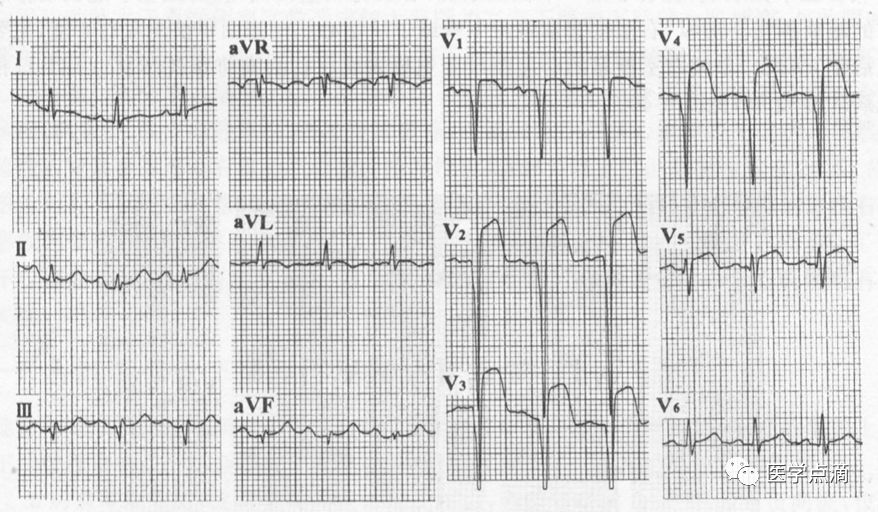
-
正常情况下,Ⅱ、Ⅲ、aVF可见,V6可见,V5、V4少见 -
Q波时相<0.04s,深度<1/4×R((同一导联)
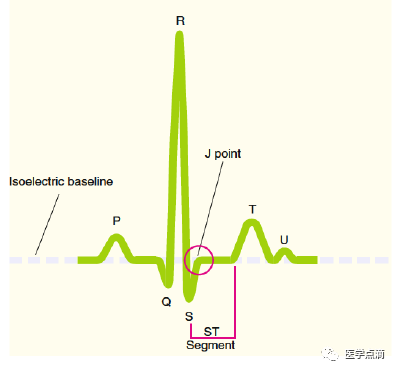
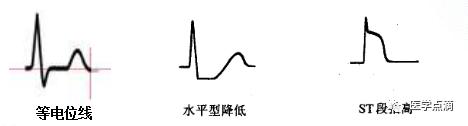
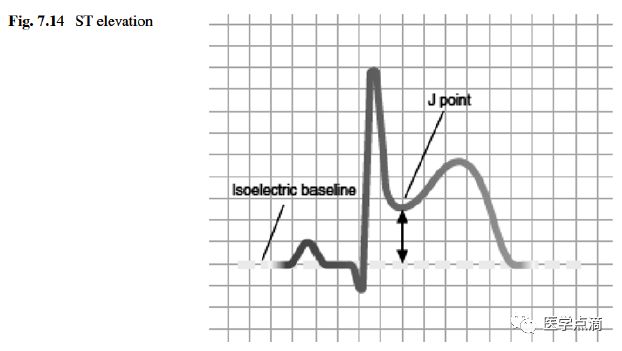
ST段移位:
-
压低:<0.05mV(ST段比基线压低>1.0mm称为ST段显著压低)
-
抬高:V1-2<0.3mV;V3<0.5mV;其他导联<0.1mV(与基线相比,ST段抬高>1mm为ST段显著抬高)

-
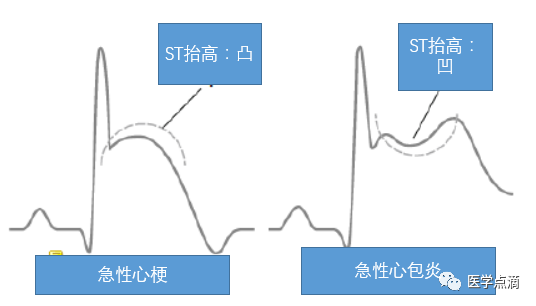
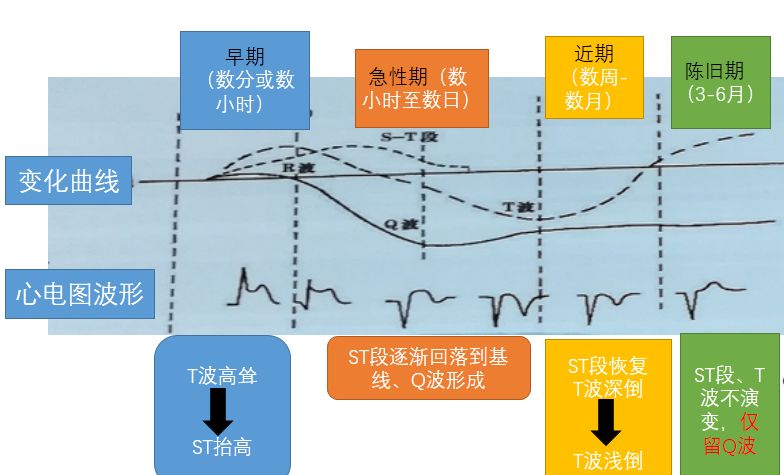
有ST段抬高:超急性(无Q波形成),急性(有Q波形成) -
无ST段抬高:陈旧性
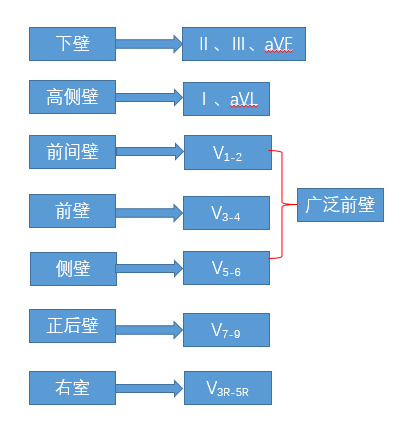
心梗定位

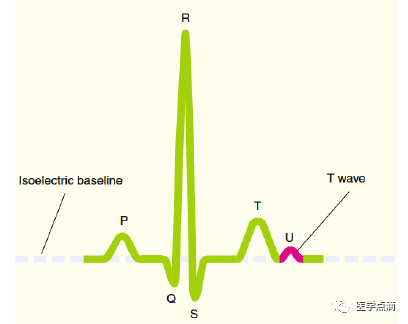
T 波

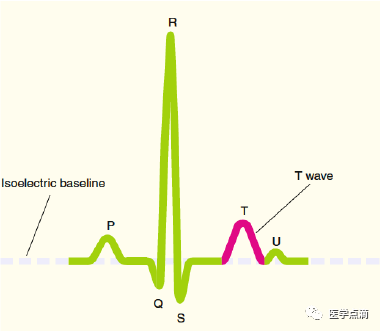
-
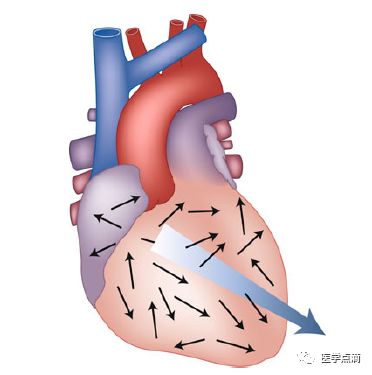
心外膜有脂肪组织包围,温度较高,可加快此处的心肌复极; -
心肌收缩时心内膜面承受的压力大,将减慢复极的进程,结果使得心室复极便自心外膜面开始,向心内膜面扩布。
早搏的鉴别

-
提前出现的P 波:P R>0.12s(房早);P R <0.12s(交界性早搏) -
提前出现的QRS波:QRS宽(室性早搏);QRS窄(交界性早搏)
-
房早伴差传:代偿间歇不完全,QRS前有P 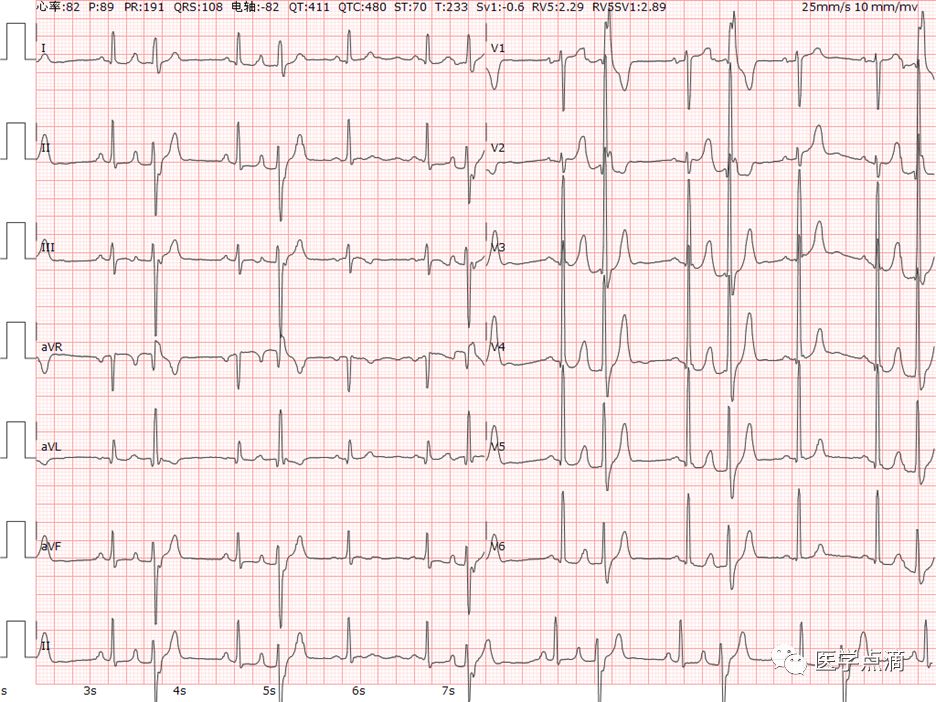
-
室早:代偿间歇完全,QRS前无相关P
心动过速(连续3次以上的早搏形成)

-
窦性心动过速(有窦性P波)(渐快渐慢)(心率:70、80、90、100、110、120)(120、110、100、90、80);窦房结折返型心动过速:突发突止。
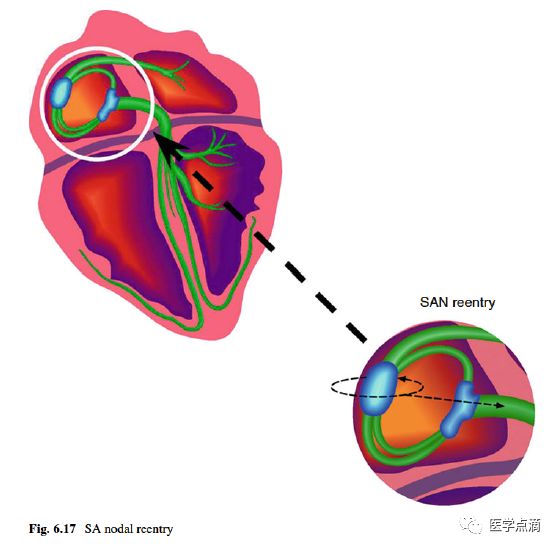
-
房性心动过速(有房性P波)(房性自律性增高型心动过速、房内折返型心动过速) -
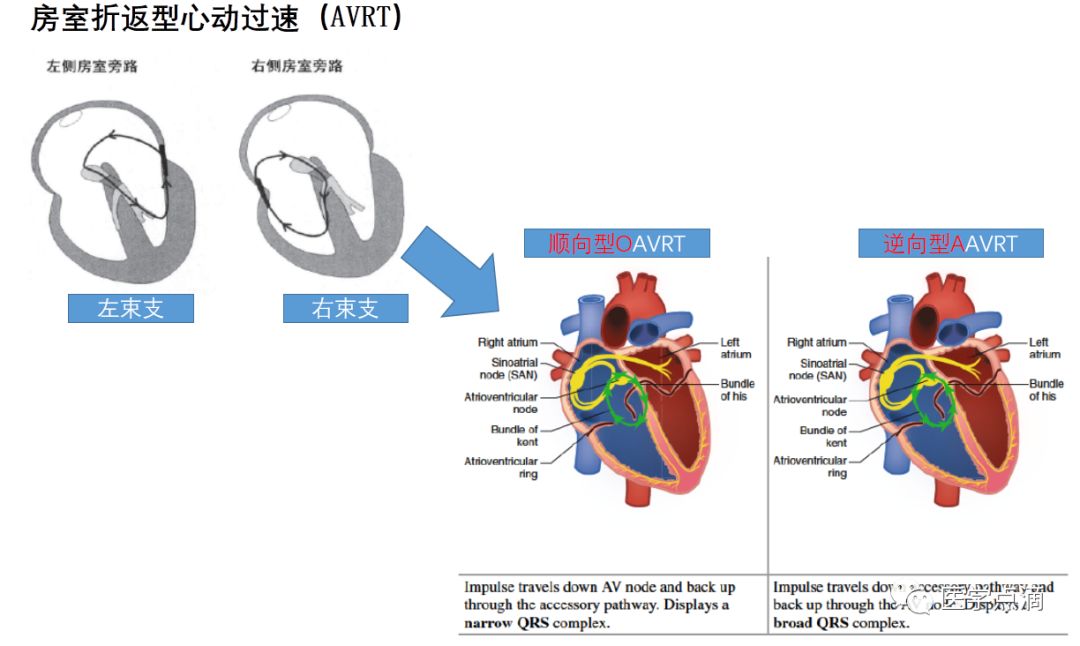
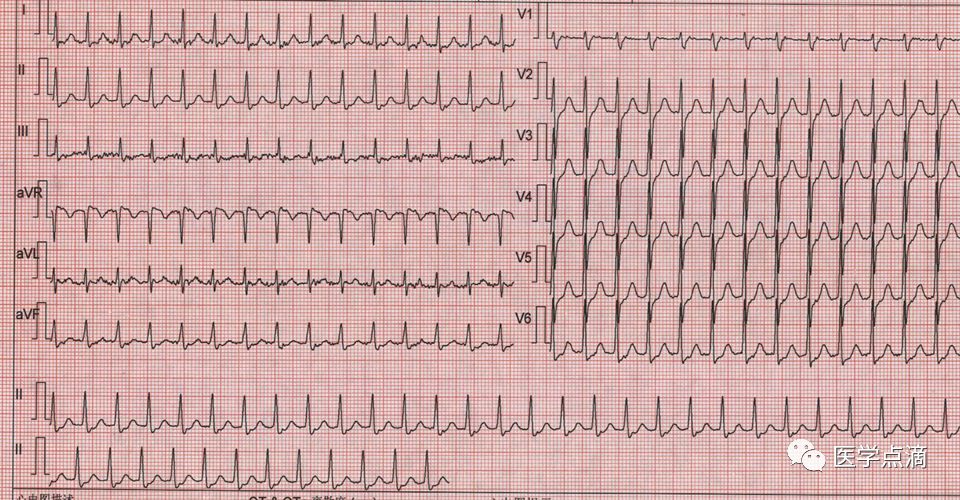
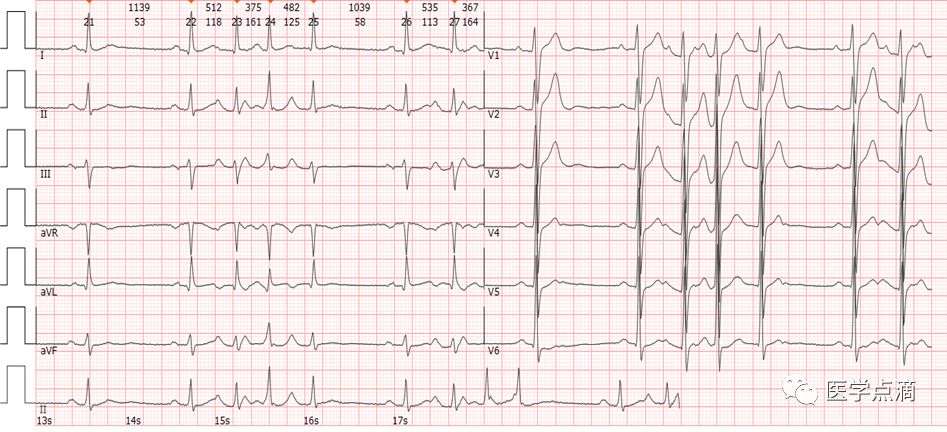
阵发性室上性心动过速(逆行P波)(分为房室结内折返型心动过速、房室折返型心动过速) 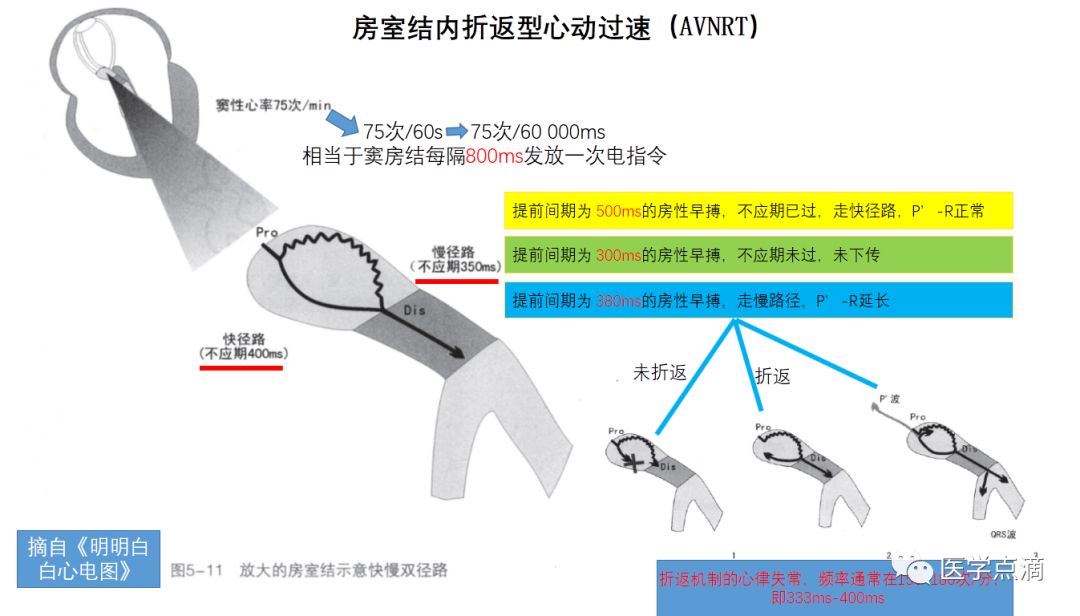
-
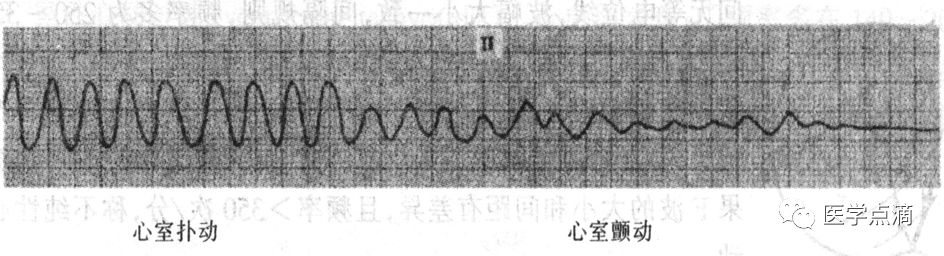
房扑(P波消失,代之F波:形态、振幅、间距都很匀齐,似锯齿样,一般在Ⅱ、Ⅲ、aVF导联上最好看)(250-350次/分)(V2、V3、aVF、V1鉴别阵发性室上速) 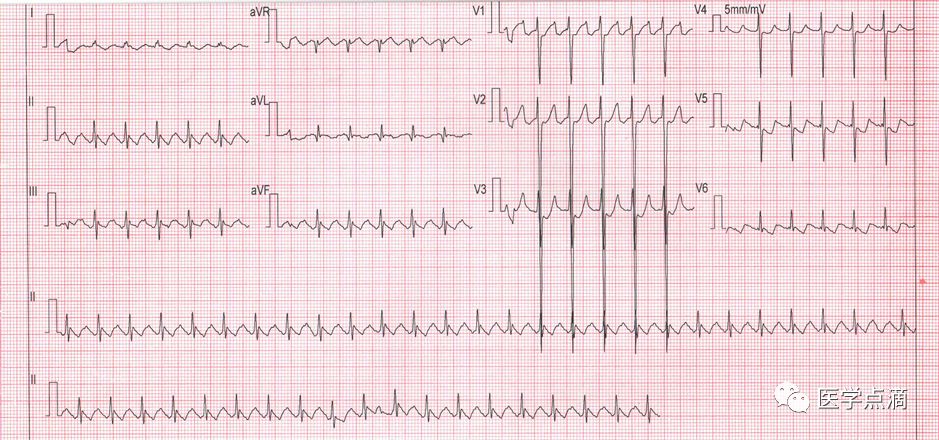
-
房颤(P波消失,代之f波:形态、间距及振幅均绝对不规则的颤动波,在V1导联上最好看)(350-600次/分) 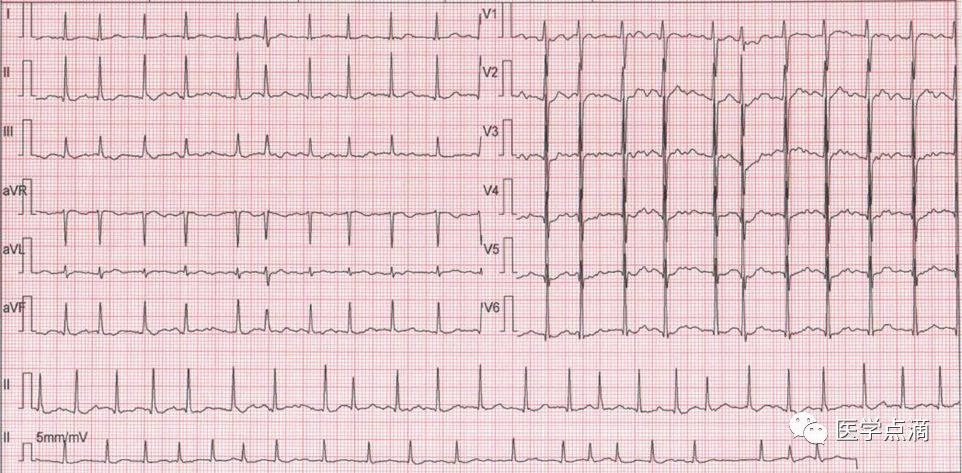
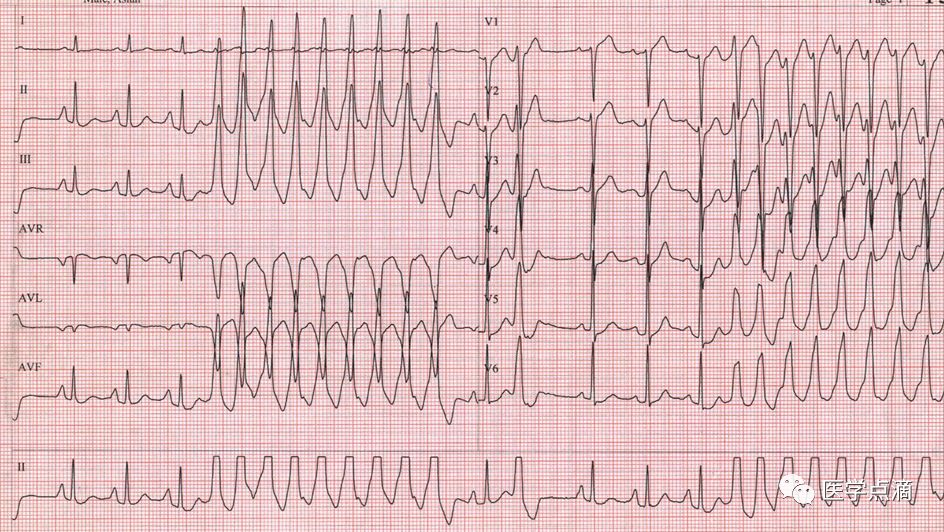
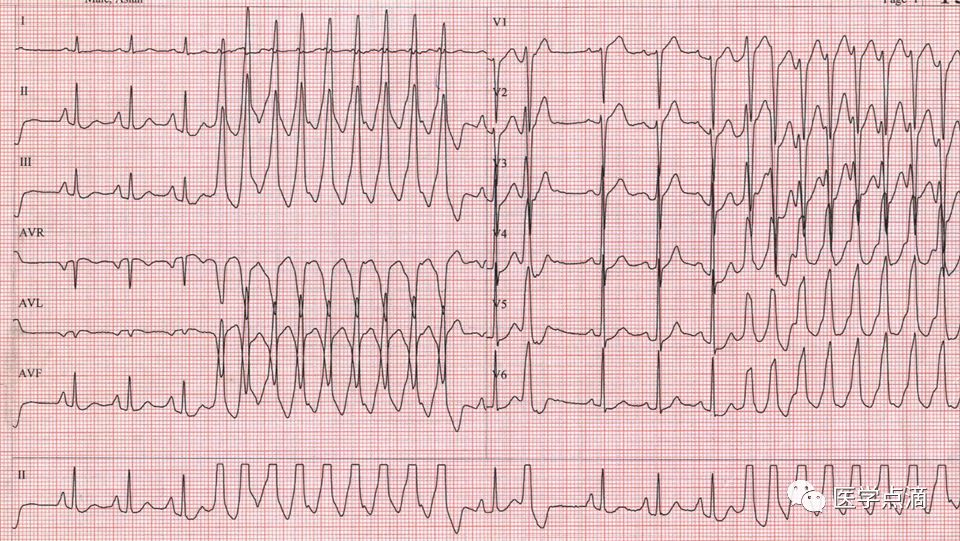
宽QRS波心动过速:
-
房速(有P 波)
-
房颤伴室内传导阻滞(不齐)
-
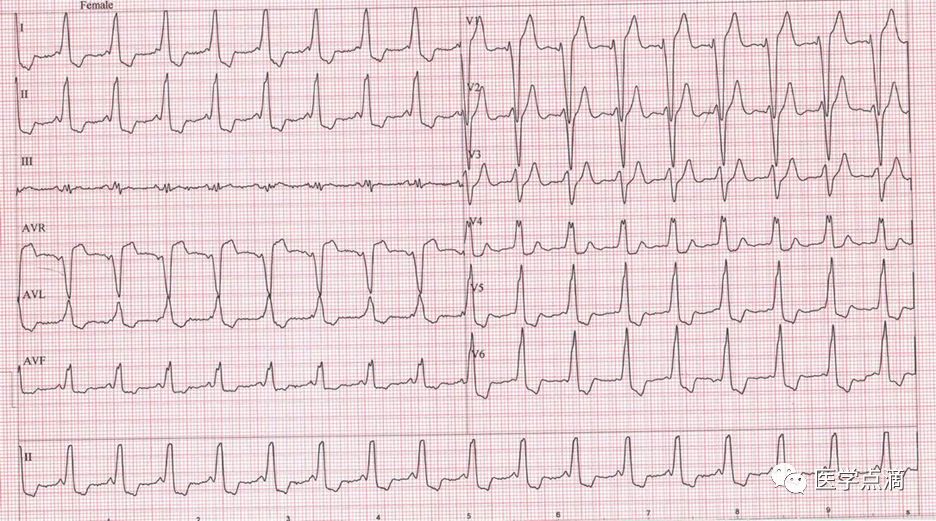
房颤伴预激(有delta波)
-
室速(最具特征的标志:房室分离、心室夺获波、室性融合波)
本文来源:医学点滴








